Child/Adolescent Orthodontics
For the Oral Health of Children
Child/Adolescent Orthodontics is a treatment modifying occlusion, tooth alignment, and jaw
bones during growth period. It reduces the probability of malocclusion. If your worry about the occlusion of
your children, please consult us first.
On the other hand, since our policy is not to perform orthodontics
too early, we do not start treatment immediately as soon as child patients come in most cases. The reason is
that children’s jaw is growing continuously, so occlusion usually get better naturally without doing anything.
It is not necessary to do over treatment. Even if the child has a true necessity to be treated, we will select
the optimal timing to start it under careful examination.
The Problem of Too Early Orthodontic Intervention
If you are the parent in Japan, you will find many surrounding children are having orthodontic treatment from 5~6 years old. This is because a method called “Syou-Kyousei”, which is performed with removable appliance, is very popular in Japan. Many dentists dedicating this method advocate that “dental arch expansion starting from early ages can prevent teeth extraction hereafter” and promote it with relatively lower price to incite parents. It is a very successful business. However, from our experience, only few children need orthodontics from such low ages. On the contrast, early orthodontic without correct knowledge may cause disaster results. Let us introduce two of them.
Elongate Treatment Span Uselessly
The dentition of child is a mixture of deciduous (milk) teeth and permanent teeth from 6 y/o to 12 y/o. If we start orthodontics from 6 y/o, it shall be finished after 12y/o that all permanent teeth are erupted. It will take more than 6 years! We can compare with adult orthodontics, which takes 2 years in average. Moreover, these 6 years is the essence of childhood. We think we should let children to grow without any orthodontic devices if possible.
Cause Impaction or Resorption of Teeth
The permanent front teeth (incisors) usually erupt on 7~8 y/o. Many parents get worried if the alignment of them is not good. However, aligning these front teeth without careful planning is very dangerous. Because there are still some tooth germs in the jaw bones, aligning incisors may block eruption path of these germs, especially upper canines. This is so-called impaction. Moreover, impacted canine sometimes goes front and absorb the root of incisors (root resorption). The most severe case of resorption cause incisor extraction.
Optimal Timing of Child Orthodontics
It is difficult to judge the timing of child orthodontics, depending on the opinions of
orthodontist. Performing orthodontics causes several disadvantages, as we have described. But on the contrast,
being afraid of these disadvantages too much may miss the best intervention timing. Diagnosis of child
orthodontics needs such precise judgement.
We hope orthodontics produces the maximal benefits to
children, thus efficient treatment without any wasting is required. This is the chance to display our ability to
the full as experienced orthodontists. We can provide optimal treatment plan with best timing for all children.
Advantages of Child Orthodontics
We have explained the risk of orthodontics. But there are still many benefits if diagnosis is accurate based on correct orthodontic knowledge.
- Guiding growth of jaw bones improve not only the tooth alignment, but the appearance of middle and lower face.
- Orthodontics performing on mixed dentition (of milk teeth and permanent teeth) can lower the burden to teeth and periodontal tissue.
- Post-treatment stability is much higher before treatment is performed on mixed dentition.
- The improvement of esthetics of face and alignment also advance social and mental health of children.
- Correction of tooth alignment improve the function of mastication and pronunciation of children.
- Having orthodontics in this era increase the consciousness to oral health.
| Child Orthodontics | Fundamental Fee |
¥330,000 |
|---|
Flow of Child Orthodontics
Child orthodontics can be divided to two parts: Stage I and Stage II treatment. The treatment goal and span are different between I and II.
Stage I Treatment
If necessary, the treatment may be started from 6~7 y/o. The aim of treatment here is not
to align teeth, but to “guide growth” of jaw bones and prepare the situation for permanent teeth eruption. After
Stage I completed, the Stage II can be performed. (Sometimes treatment will be all completed only with Stage I.)
Treatment span: 1~2 years
Frequency of visit: once in 1~3 months
Stage II Treatment
Treatment performed after the permanent teeth are erupted (about 12 y/o). This the
so-called orthodontics to align teeth and is almost equal to adult orthodontics. Finishing, detailing, and
building esthetical dentition is the goal in this stage.
Treatment span: 1~3 years
Frequency of
visit: once in a month
“Stage I combined with Stage II” vs. “Stage II only” (= adult orthodontics)
- If the child patient has the problem of “skeletal inharmony”, which is the severe divergence
between upper and lower jaw bones, performing Stage I at first can correct this inharmony with bone growth guidance effectively. The problem of alignment can be also solved easily at stage II. On the contrast, if patient with large bone divergency miss this timing of growth modification, treatment result will be compromised with adult orthodontics. Moreover, if the inharmony is too severe, orthognathic surgery need to be considered to fix the problem. - On the other hands, if skeletal inharmony is limited, we do not need to have aggressive stage I treatment. Waiting after all permanent teeth erupted and having Stage II directly is acceptable in these slighter cases.
Optimal Treatment Timing Judgement
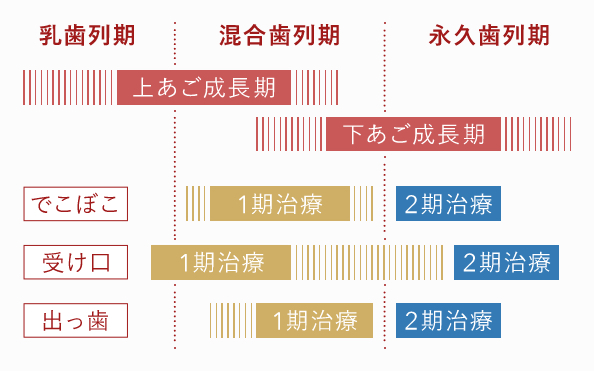
As the left figure, the optimal timing of three different malocclusion cases is shown. Correct intervention
timing should be judged basing on skeletal type, occlusal type, permanent teeth eruption, growth stage, and
growth spurt.
(乳歯列期:milk teeth dentition; 混合歯列期:mixed teeth dentition; 永久歯列期:permanent teeth
dentition; 上あご成長期:upper jaw growth; 下あご成長期:lower jaw growth; でこぼこ: crowding dentition; 受け口: protruding lower
jaw; 出っ歯:protruding upper jaw)
Growth Spurt
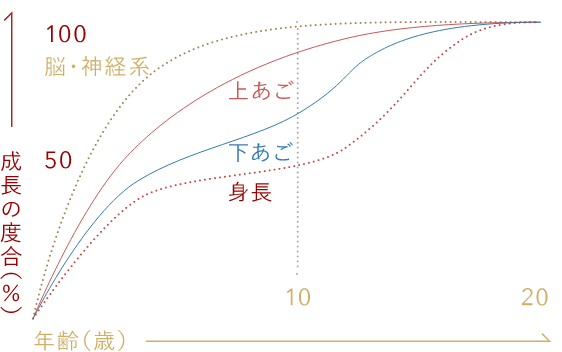
The spurt of growth is different depending on different parts of body and sexuality.
脳神経系:
Head
Since the growth spurt of head (equal to the brain) is very early, abnormity of head should also
be treated very early. But there is little relationship with orthodontics.
上顎骨: Upper jaw bone
The growth spurt is 5~8 y/o. This is earlier because it is closer to the head. The growth will be
all finished before 10 y/o.
下顎骨: Lowe jaw bone
The growth of lower jaw is similar to the body
height (身長= body height), and is much later than upper jaw.The effect of sexuality
Generally, girls
have growth spurt earlier than boys. Thus, girls should be treated earlier.
Protruding Upper Jaw
Need to restrain the growth of upper jaw and facilitate lower.Stage I is performed at 8~10 y/o, and stage II is 11~13 y/o.
Protruding Lower Jaw
The main way to fix this problem is to facilitate growth of upper jaw. So, most cases have to be treated from 6~8 y/o. Stage II should be started at about 12~16 y/o that the growth of lower jaw has been finished.
Snaggletooth (Crowding)
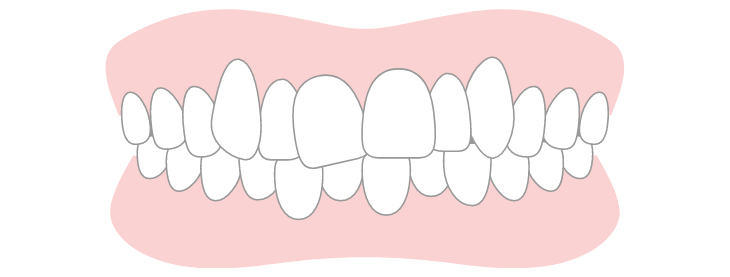
This problem is caused by the space discrepancy of large tooth size and small jaw size. If this discrepancy is slighter, we can expand dentition to create space from late mixed dentition (8~10 y/o). But in most cases, we can also wait until all permanent are erupted and have only Stage II treatment directly.
Projecting Teeth (Bimaxillary protrusion)
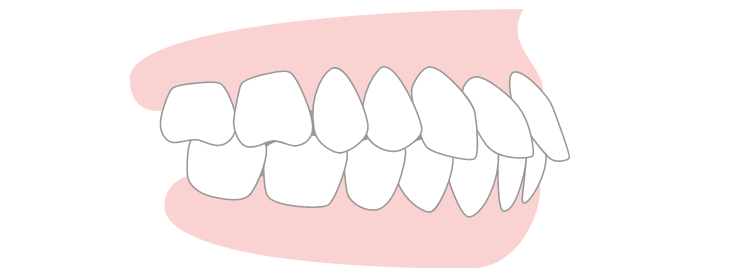
It is necessary to clarify the cause is skeletal or dental. The skeletal problems can be considered to be approached from Stage I. Usually it is started from 8~10 y/o. On the other hands, if the problem is dental, we can have Stage II treatment only after permanent teeth erupted.
Open Bite
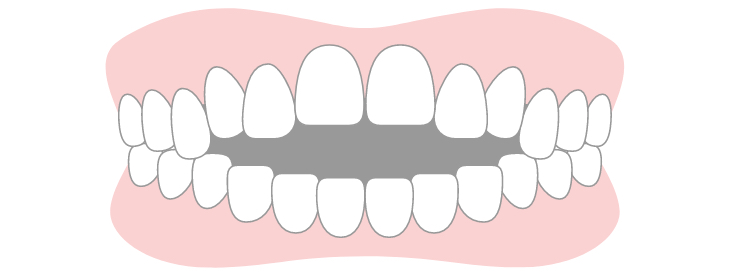
The cause of open bite is various. If it is caused by bad habit, in most cases tongue thrusting, MFT (muscle functional treatment) can be performed from 6~8 y/o.
Deep Bite
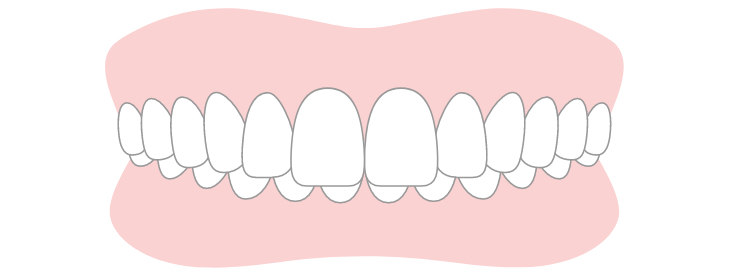
It is necessary to promote the growth of lower jaw, and should be started from 8~10 y/o. Stage II may be started at 11~13 y/o.
Side Shift of Jaw Bones and Teeth
It should be treated synchronizing to both upper and lower jaw growth. Generally, it is treated earlier, from 8~10 y/o. Moreover, treatment usually elongate since it must be finished until the growth of lower jaw completed.
Pay Special Attention to Your Child’s “This Tooth”
The following situations should actually be given more attention than irregularities such as crooked or protruding teeth. Parents themselves and general dentists often fail to notice these, so we recommend early “consultation” with an orthodontic specialist. However, we repeat, even if such conditions exist, do not rush into orthodontic treatment without carefully evaluating the risks and benefits of the treatment and then deciding on the appropriateness of orthodontic intervention.
Impacted Teeth (Maifukushi)
There are teeth that are delayed in eruption or remain “buried in the bone” due to lack of space for eruption,
abnormal position of the tooth bud, or the influence of supernumerary teeth.
Especially in children’s mouths, this commonly occurs in the upper front teeth, canines (the third tooth from
the front), and wisdom teeth (third molars). Particularly, impaction of the upper canine, as mentioned in the
previous paragraph, also carries the risk of resorbing the roots of the front teeth. Our clinic uses dental CT
to accurately determine the position of the impacted teeth and predict the direction of eruption, and we provide
orthodontic treatment to correct the direction of eruption and ensure space for the teeth to emerge properly.
Supernumerary Teeth (Kajoushi)
“Supernumerary teeth,” where more teeth are formed than the usual number, are commonly found in children’s
mouths.
Some are already erupting, while others remain buried in the gums (impacted supernumerary teeth). Especially,
impacted supernumerary teeth can delay the eruption time of adjacent permanent teeth, cause gaps in the teeth
(diastema), and, in the worst cases, also pose a risk of root resorption. When future impact is considered, we
remove them at the appropriate time while caring for the child’s psychological well-being.


